
|Articles|March 16, 2016
Where You Want It, When You Need It: Point of Care Ultrasound
Author(s)Jason Birnholz, MD
Embracing the portability of point of care ultrasound.
Advertisement
On the Practice of Ultrasound
Fellow Ultrasounders,
I am happy and honored to continue my column at Diagnostic Imaging, which is one of the most respected online publishers for the global medical imaging community. I have the same feeling of pride I recall on moving from Assistant Professor at Stanford to Associate Professor at Harvard. I did my first editorials for DI when I was a full professor in the 1980s, so it’s a lot like coming back home, albeit to a freshly refurbished place with friendly neighbors.
The reach of DI is broad, so some of you may not know about my original 25 articles on
I like to work at the Intersection (big I) of patient, pathology, examiner, equipment, and knowledge. The big I is not a singularity but an evanescent mote skipping along an irregular, Brownian arc in hyperspace as we learn, as general knowledge increases, and equipment performance improves.
This first DI column more or less coincides with the start of the next AIUM. I have selected a new horizon in portable ultrasound exams because of the equipment that will be introduced by the Sonoscanner Company. Abstracts of AIUM’s upcoming oral presentations, representing a vast amount of work and confirming how truly ultrasound has come of age as a science-based, clinical endeavor.
House Calls
Ultrasound has an awesome range of clinical utility. Most of its detractors harp on how subjective it is, but that can be a strength when education, experience, and equipment coalesce.
I have been enabled to do house calls, as well as providing diagnostic assistance at public health clinics. One recent case was as a ‘reassurance’ exam for an elderly primipara in the late third trimester who had an ‘irregular heartbeat’ in an office ultrasound and a ‘normal’ fetal echocardiogram a week later. The ultraportable study revealed mild growth retardation, a very tight nuchal cord, and early signs of compromised condition. Cerebral periventricular cortex was normal. The cervix was not inducible; delivery was by C-section with a good outcome but required a NICU admission.
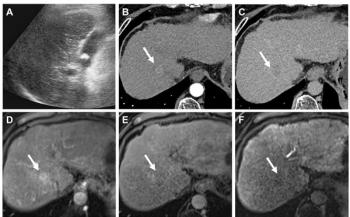
Another case was a 64-year-old woman with a prior history of rotator cuff tears. She had progressive and incapacitating shoulder pain and an extremely limited range of motion for four months. Early in the course of this episode, she had a shoulder ultrasound by an orthopedist who based the plan of therapy on a normal appearance of that study and prior knowledge of the patient. The bedside look showed the crenated surface pattern of avascular necrosis of the humeral head with two avulsed fragments. An MRI was requested from a radiology facility after which a shoulder replacement was performed.[[{"type":"media","view_mode":"media_crop","fid":"46922","attributes":{"alt":"","class":"media-image media-image-right","id":"media_crop_9813949582920","media_crop_h":"0","media_crop_image_style":"-1","media_crop_instance":"5484","media_crop_rotate":"0","media_crop_scale_h":"0","media_crop_scale_w":"0","media_crop_w":"0","media_crop_x":"0","media_crop_y":"0","style":"height: 543px; width: 400px; border-width: 0px; border-style: solid; margin: 1px; float: right;","title":"Figure 1. The humeral head has a grossly irregular contour, an avulsed bone fragment is seen in the lower section.","typeof":"foaf:Image"}}]]
Low-end and New Market Disruption
I was chatting in very general terms about my house call experiences when a business woman said that this is ‘disruptive technology’. I disagreed. The equipment was a pleasure to use, it made my work smoother. Also, I was thinking that no one doing scans wants disruption in any form, or any other rupt for that matter. We tend to have too much on our plates as it is. Her response was, ‘go read
As I understand it, a lot of people refer to disruptive technology, but the concept applies specifically to business models, not products or services themselves. A low-end disruption is a plan that aims to provide something for an underserved market or one that is unable to be served with an existing form of technology (mainly because it is not profitable for incumbent manufacturers to do so). The disruptive product is typically cheaper than the existing one and will have fewer features (ie, a no-frills, simple to use package). It may also have shoddier construction, less reliability, or poorer performance, although it is also possible that it is a true technologic advance in concept or fabrication. In either case, incumbent companies will be as quick to point out the supposed lethal flaws of ‘cheaper’ as they are to extol the virtues of their own solutions. This was beginning to sound very familiar to me.
When I was acquiring information about portable devices for another review, I was put in contact with the in-charge person, who was almost always a business leader, typically one with a technical, not medical, background. This is important, because the commercial outlook is to define the ‘underserved’ market as a buyer of the device. I heard a lot about plans to sell equipment to practitioners in India, Brazil, and for the US and Europe, to physicians and clinics with no current ultrasound availability or experience. The thought seems to be that a little limited performance ultrasound is certainly better than none, that malpractice is not an issue, and that there is no conflict in this usage with an unremitting fee for service usage.
To us, the ‘underserved’ are patients, and therein lies a nearly impenetrable gap. If you know how to scan, it is unethical to knowingly use inferior equipment, except when there is truly no other alternative. For a large department with a lot of examining rooms, I think of this as the upgrader’s dilemma. Using subjective-intense diagnostic equipment without adequate training is also contrary to best medical practices.
Progress
I was very impressed with the Sonoscanner U-Lite when I reviewed it initially. Since then, it has expanded its initial four transducer set, added several apps for quantitative analysis, and done further software tweaking and noise reduction. This is the version to be introduced at AIUM. The U-Lite has its own path towards image synthesis, technically, I suppose, between phase correcting beam former systems and plane wave insonification. The U-Lite has full system performance in a 600 gram package with a high definition touch tablet display. I am a big fan of plane wave insonification for a fixed location unit. It will be an interesting race between miniaturizing a fully operational plane wave device and further development of the unique form of image synthesis of the Sonoscanner. (Note: I’m waiting for Sonoscanner to name their processing scheme, so I can refer to it generically.) All of us as scanners will benefit, however this goes.
How
The primary issue with any portable device is how it is to be used. Business disruptors tend to focus on single use applications of ultrasound. This might be a screening for just one form of pathology or as an aid to one procedure, like guidance for needle placement/aspiration/biopsy or automated determination of bladder volume. The operational problem is that patients are not at all ‘standardized’. I like to keep thinking vive la difference, but it is usually easier to evaluate a slender patient than someone with a massive BMI.
Another option is a limited exam for different parts of the body on different patients. This is what goes on most of the time. It is an easy conceptual transition from a fixed location set up to mobile and various preventive medicine screenings when equipment performance is essentially the same.
The most demanding option is to use ultrasound as a physical exam, where the extent and thoroughness are governed solely by the clinical issues that pertain. This approach yields the most actionable information that can be achieved with ultrasound, but it means the examiner has to know all about patients, equipment, imaging, and diseases and to keep their personal big I’s moving; equipment performance really has to be great.
Who[[{"type":"media","view_mode":"media_crop","fid":"46853","attributes":{"alt":"Jason Birnholz, MD","class":"media-image media-image-right","id":"media_crop_827790522229","media_crop_h":"0","media_crop_image_style":"-1","media_crop_instance":"5466","media_crop_rotate":"0","media_crop_scale_h":"0","media_crop_scale_w":"0","media_crop_w":"0","media_crop_x":"0","media_crop_y":"0","style":"height: 299px; width: 200px; border-width: 0px; border-style: solid; margin: 1px; float: right;","title":"Jason Birnholz, MD","typeof":"foaf:Image"}}]]
Effective ultrasound usage is not about whether it is done by a physician or technologist. Business disruptors tend to focus on physicians for low performance devices with the assumption that they can leverage their knowledge of pathology quickly. The problem with that is that that applying that knowledge requires excellent image quality, so it will only work under some circumstances. At the hard end of the practice spectrum, technologists who were educated near the start of high speed ultrasound era grew up in a framework of systemic medical diagnoses. They have accrued the practical experience to cope with a full range of what may be encountered in their daily practices. The comfort range and trajectory of the big I are individual and title independent.
Where
I am pretty sure that the best and most easily implemented initial uses of high performance ultraportable ultrasound are in medium and large hospital settings. That’s where you have a concentration of sick people, residents, and fellows being trained in ultrasound, and staff who are, presumably, experienced. Let me give you a few examples: A gynecology resident has a clinic day. He or she thinks there is a palpable abnormality and whips the unit out of a pocket, tote bag, or backpack, attaches the endovaginal probe and does the exam then and there. That’s efficiency. If more imaging needs to be done, there are always the fixed location units, whose own schedules will not be perennially clogged by the shot gun approach to imaging diagnostics.
Another example is the endocrine fellow, who uses the unit and finds a thyroid nodule with microcalcifications and a central vascular pattern. As soon as the procedure is explained and the paper work executed, there can be an instant guided needle aspiration biopsy. A vascular surgeon should want to have a vascular ultrasound technologist in the OR doing continuous peripheral artery flow quantitation to insure procedure effectiveness and decrease restenosis rates; and how about follow-up looks after transplant surgery, chemotherapy, or a sports injury?
I think that every radiology department should issue all of its new residents with ultraportable units. There is nothing that will better teach what imaging is all about than immersive ultrasound use when it really counts. Everything that you learn about imaging any part of the body applies to all other ways that you can look at the same region.
Coda
Small ultrasound units have been around ultrasound for a long time, none of which have had much traction until the last few years. Laptop and platform units have become popular, but they have not replaced high-end units, even though with some manufacturers, image formation and processing is identical in units with different configurations and different pricing. We are now at the start of an era with ‘high performance’ features shrunk into physically small units. I can’t even compare my first 10+ years of personal computers with what my smart phone does now, and I shouldn’t be able to either. Ditto for ultrasound.
Forget about disruption, it’s not medically appropriate. Think efficiency and about how we can deliver our imaging services in a way that respects the needs of the patients we serve. The point of care is where we do our thing, and that is now anywhere.
Newsletter
Stay at the forefront of radiology with the Diagnostic Imaging newsletter, delivering the latest news, clinical insights, and imaging advancements for today’s radiologists.
Advertisement
Related Content
Advertisement

Latest CME








Advertisement
Advertisement
Trending on Diagnostic Imaging
1
FDA Clears AI-Powered Triage Platform for Digital Breast Tomosynthesis
2
Leading Breast Radiologists Discuss the Recent Lancet Study on AI and Interval Breast Cancer
3
Is AI Better Than Neuroradiologists at Evaluating Aneurysm Growth on CTA and MRA Scans?
4
Radiology Roundup of New FDA Clearances — February 1 — February 7
5