
|Articles|April 1, 2007
Ultrasound checks out suspicious neck lumps
Modern high-resolution ultrasound has excellent spatial and contrast resolution for the near field, and the development of 3D technology, extended field-of-view or panoramic imaging, and color flow and power Doppler applications has led to great improvements in its diagnostic utility and accuracy.
Advertisement
Ultrasound is the second most common method of imaging carried out in hospitals worldwide after plain-film radiography. Modern high-resolution ultrasound has excellent spatial and contrast resolution for the near field, and the development of 3D technology, extended field-of-view or panoramic imaging, and color flow and power Doppler applications has led to great improvements in its diagnostic utility and accuracy. The technology involves no ionizing radiation, is readily available in most centers, and is relatively inexpensive compared with CT, MRI, and PET.
The superficial nature of the neck structures lends itself readily to ultrasound assessment, and ultrasound plays an increasingly important role in head and neck imaging. Ultrasound can provide reliable real-time guidance for fine-needle aspiration cytology (FNAC) or core biopsy, and recognition of its versatility and diagnostic accuracy has led to its routine incorporation in head and neck clinics.
A patient presenting with a neck mass is a common clinical scenario. A meticulous clinical history with physical examination usually provides a reasonable clinical diagnosis. Imaging is necessary for accurate diagnosis and assessment of the extent of a lesion's involvement prior to treatment.
High-resolution ultrasound is an ideal initial imaging investigation for most neck lumps.1 Cross-sectional modalities serve a supplementary role, offering accurate presurgical anatomic localization, particularly for more deep-seated and locally extensive lesions. The differential diagnosis of a neck mass depends on a patient's age, the anatomic location of the lesion, and its appearance on ultrasound. Lesions in the head and neck are site-specific (see table), and practitioners should familiarize themselves with the locations of common lesions and their imaging characteristics.
The basic level of equipment required for head and neck ultrasound is a modern system with a high-frequency transducer ( > 7.5 MHz). High-frequency transducers allow excellent near-field resolution, though they are not as good at visualizing deeper structures. Lower frequency transducers (5 MHz) may occasionally be required for assessing deep-seated lesions, such as those in the deep lobe of the parotid gland.
Color flow imaging is now a routine part of the ultrasound examination. Systems should ideally offer high-sensitivity color-flow imaging and power Doppler functionality. Equipment used for functional imaging should be calibrated to depict slow-flowing vessels in the head and neck without artifacts or background noise caused by oversensitivity. The lingual artery in the floor of mouth is a useful and practical vascular landmark for calibration.
We recommend the following for power Doppler examinations: high sensitivity, low wall filter, pulse repetition frequency of ~700 Hz, and medium persistence.
The patient should be positioned with the neck slightly extended. Placing a pillow behind the shoulders and lower neck allows the patient to adopt a comfortable position that can be maintained throughout the examination.
An easily replicated systematic scanning protocol is essential. We routinely evaluate the following regions consecutively: submental, submandibular, parotid, upper cervical, midcervical, lower cervical, supraclavicular fossa, posterior triangle, and midline of the neck (including the thyroid gland).2
Scanning in a transverse plane is adequate in most circumstances. Supplementary examination in longitudinal and oblique planes helps to delineate the lesion and its relationship with adjacent anatomic structures.
LIKELY LUMPS
Because most lesions in the neck are site-specific, once a lesion has been located, specific ultrasound features can be used to establish the diagnosis. This can be confirmed from ultrasound-guided FNAC, allowing appropriate clinical management and treatment.
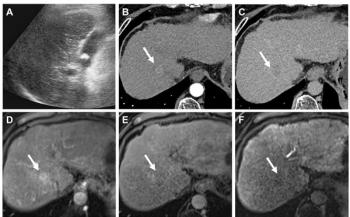
- Lymph nodes. An enlarged cervical lymph node is the most commonly encountered neck lump. The role of ultrasound is to differentiate pathological nodes (e.g., metastases, lymphoma, tuberculous lymphadenitis) from normal/reactive nodes (Figure 1). Different ultrasound criteria have been established to differentiate benign from malignant cervical lymph nodes.3 No single criterion is an absolute indicator for predicting malignant nodal disease, and all known ultrasound criteria should be applied together. These signs may point to a specific diagnosis or help determine which lymph node to sample using ultrasound-guided FNAC.
Size alone is a poor criterion. Among the various measurement parameters for nodal size, minimum axial diameter is the most specific dimension for predicting malignancy. Van den Brekel et al recommend a minimum axial diameter of 7 mm for submental/submandibular nodes and 8 mm for other cervical nodes.4 They cite an overall accuracy of 70% when minimum axial diameter is used as a sole diagnostic criterion. If ultrasound examination of a patient with head and neck cancer reveals a lymph node that is increasing in size or new nodes, then these findings should be viewed with a high degree of suspicion.
Malignant lymph nodes are commonly round, while benign nodes tend to have an elliptical shape.5-7 Axis ratios (either short/long or long/short) can be measured, though a visual qualitative assessment is usually sufficient.
The presence of an echogenic hilus within a cervical lymph node reflects preserved sinusoidal architecture and is a good sign for predicting benignity.8,9 The presence of a round node with an absent hilus is highly indicative of malignancy.
A diffusely hypoechoic, or pseudocystic, enlarged lymph node has previously been described as a sign of lymphoma. Newer generation transducers, however, more commonly show a reticulated intranodal pattern.10,11
In patients with primary squamous cell carcinoma (SCC), the presence of necrosis (coagulative and cystic) within an enlarged lymph node is a very strong indicator of malignancy.12 Tuberculous nodes and metastases from papillary thyroid carcinoma also tend to undergo cystic degeneration,13 and these may mimic metastatic nodes from SCC. An ill-defined border or frank invasion of neighboring structures can be detected easily with ultrasound and indicates poor prognosis.
On color Doppler imaging, the distribution of vessels within a node is more reliable than various vascular and resistive indices.14 Benign nodes have a central hilar flow pattern, whereas malignant nodes have a disorganized peripheral pattern. Areas of relative avascularity reflect the presence of necrosis and peripheral subcapsular vessels.14-17
The typical small punctate calcification seen in a papillary thyroid carcinoma is also observed in lymph node metastases from papillary carcinoma.18 The sign is specific and should prompt a diligent search for the thyroid primary.
- Second branchial cleft cyst. Ninety-five percent of all branchial cleft anomalies arise from remnants of second branchial apparatus. Second branchial cleft cysts are most common in children and young adults, and the anatomic location is one of the best clues for diagnosis. These cysts are generally found superficial to the common carotid artery and internal jugular vein, posterior to the submandibular gland, and along the medial and anterior margin of the sternocleidomastoid muscle.
Appearance on ultrasound depends on whether there is any previous infective or hemorrhagic component.19 Most uncomplicated branchial cleft cysts appear as well-circumscribed round/ovoid anechoic masses with thin walls and posterior acoustic enhancement. Some cysts may exhibit a pseudosolid appearance due to the presence of cellular material and cholesterol. Previous episodes of infection or hemorrhage may cause the lesions to appear ill defined and thick walled, with septae and heterogeneous internal echoes (Figure 2). Lesions with this appearance should be differentiated from metastatic lymph nodes. Further evaluation will require ultrasound-guided FNAC.
- Thyroglossal duct cyst. This congenital anomaly is related to the thyroglossal duct. Most lesions are anatomically related to the hyoid bone. About 25% to 65% occur in the infrahyoid neck, 15% to 50% occur at the level of the hyoid, and 20% to 25% are suprahyoid. Thyroglossal duct cysts are characteristically located in the midline of the anterior neck above the thyroid cartilage. The cysts are slightly off midline and deep to strap muscles at the level of thyroid cartilage.
Thyroglossal duct cysts typically appear on ultrasound as well-defined thin-walled anechoic cysts with posterior acoustic enhancement (Figure 3). They may have a uniformly pseudosolid echo pattern similar to branchial cleft cysts, owing to proteinaceous content. Previous infection or hemorrhage can result in a heterogeneous appearance.20
The role of ultrasound in patients diagnosed clinically with a thyroglossal duct cyst is to confirm diagnosis and the cyst's relation to the hyoid bone, to detect internal solid components suspicious for malignancy, and to detect the presence of normal thyroid tissue in the neck. If the only functioning thyroid tissue is contained within the thyroglossal duct cyst, then surgery may result in hypothyroidism.20
- Lipoma. This benign encapsulated fatty lesion is typically subcutaneous or submucosal in location. About 13% of all lipomas occur in the head and neck. The typical appearance on ultrasound is a well-defined compressible avascular/hypovascular hypoechoic mass with linear echogenic streaks parallel to the transducer (Figure 4).21
- Nerve sheath tumor. Schwannoma and neurofibroma are the most frequently encountered nerve sheath tumors in the head and neck. Common sites in the neck include the vagus nerve, ventral and dorsal cervical nerve roots, cervical sympathetic chain, and brachial plexus. Nerve sheath tumors appear as well-defined solid heterogeneous hypoechoic masses on ultrasound (Figure 5). The presence of a thickened nerve continuous with the mass is the best clue.22 The nerve sheath tumor is typically hypervascular on power Doppler examination.
- Venous vascular malformation. Approximately 15% of venous vascular malformations occur in the head and neck region. Malformations appear as well-defined heterogeneous hypoechoic masses on ultrasound. Multiple sinusoidal spaces containing slow-flowing internal echoes are also seen (Figure 6).23 The presence of phleboliths (small echogenic foci with posterior acoustic shadowing), seen in about 20% of cases, essentially confirms diagnosis.
- Lymphangioma. Most lymphatic malformations develop and present in childhood. Lymphangiomas in infants are commonly located in the posterior triangle and cervicothoracic junction, whereas in adults they are found in submental, submandibular, and parotid regions. A characteristic feature of large lymphangiomas is their transpatial distribution.
Macrocystic lymphangioma appears on ultrasound as a multiseptated compressible thin-walled cystic lesion (Figure 7). Intervening infection or hemorrhage may produce thick-walled lesions with poorly defined contours and internal echogenic debris. Although ultrasound is a useful diagnostic tool that guides sclerotherapy treatment, either CT or MRI will be required to map the entire anatomic extent of large lymphangiomas.
High-resolution ultrasound is an ideal initial imaging investigation for patients with a neck lump to characterize the lesion and delineate the anatomic extent of involvement. It can provide real-time guidance for safe FNAC or biopsy to enhance diagnostic accuracy. This information will generally be sufficient for guiding appropriate clinical management.
Dr. Wong and Dr. Lee are radiologists, Prof. King is professor, and Prof. Ahuja is department head, all in the department of diagnostic radiology and organ imaging at the Chinese University of Hong Kong. Dr. Ying is an associate professor in the department of health technology and informatics at the Hong Kong Polytechnic University.
References
- Ahuja AT. Lumps and bumps in the head and neck. In: Ahuja AT, Evans RM, eds. Practical head and neck ultrasound. London: Greenwich Medical Media Limited, 2000:87-104.
- Evans RM. Anatomy and technique. In: Ahuja AT, Evans RM, eds. Practical head and neck ultrasound. London: Greenwich Medical Media Limited, 2000:1-16.
- Evans RM, Ying M, Ahuja AT. Ultrasound. In: Ahuja AT, Evans RM, King AD, van Hasselt CA, eds. Imaging in head and neck cancer: a practical approach. London, Greenwich Medical Media Limited, 2003:3-16.
- van den Brekel MW, Castelijns JA, Stel HV, et al. Occult metastatic neck disease: detection with US and US-guided fine-needle aspiration cytology. Radiology 1991;180(2):457-461.
- Vassallo P, Wernecke K, Roos N, Peters PE. Differentiation of benign from malignant superficial lymphadenopathy: the role of high-resolution US. Radiology 1992;183(1):215-220.
- Ying M, Ahuja A, Brook F, et al. Sonographic appearance and distribution of normal cervical lymph nodes in a Chinese population. J Ultrasound Med 1996;15(6):431-436.
- Ahuja A, Ying M, King W, Metreweli C. A practical approach to ultrasound of cervical lymph nodes. J Laryngol Otol 1997;111(3):245-256.
- Solbiati L, Rizzatto G, Bellotti E, et al. High-resolution sonography of cervical lymph nodes in head and neck cancer: criteria for differentiation of reactive versus malignant nodes. Radiology 1988;169(P):113.
- Rubaltelli L, Proto E, Salmaso R, et al. Sonography of abnormal lymph nodes in vitro: correlation of sonographic and histologic findings. AJR 1990;155(6):1241-1244.
- Ahuja A, Ying M, Yang WT, et al. The use of sonography in differentiating cervical lymphomatous lymph nodes from cervical metastatic lymph nodes. Clin Radiol 1996;51(3):186-190.
- Ahuja AT, Ying M, Yuen HY, Metreweli C. 'Pseudocystic' appearance of non-Hodgkin's lymphomatous nodes: an infrequent finding with high-resolution transducers. Clin Radiol 2001;56(2):111-115.
- Som PM. Lymph nodes of the neck. Radiology 1987;165(3):593-600.
- Ying M, Ahuja AT, Evans R, et al. Cervical lymphadenopathy: sonographic differentiation between tuberculous nodes and nodal metastases from non-head and neck carcinomas. J Clin Ultrasound 1998;26(8):383-389.
- Ahuja AT, Ying M, Ho SS, Metreweli C. Distribution of intranodal vessels in differentiating benign from metastatic neck nodes. Clin Radiol 2001;56(3):197-201.
- Ariji Y, Kimura Y, Hayashi N, et al. Power Doppler sonography of cervical lymph nodes in patients with head and neck cancer. AJNR 1998;19(2):303-307.
- Wu CH, Chang YL, Hsu WC, et al. Usefulness of Doppler spectral analysis and power Doppler sonography in the differentiation of cervical lymphadenopathies. AJR 1998;171(2):503-509.
- Na DG, Lim HK, Byun HS, et al. Differential diagnosis of cervical lymphadenopathy: usefulness of color Doppler sonography. AJR 1997;168(5):1311-1316.
- Ahuja AT, Chow L, Chick W, et al. Metastatic cervical nodes in papillary carcinoma of the thyroid: ultrasound and histological correlation. Clin Radiol 1995;50(4):229-231.
- Ahuja AT, King AD, Metreweli C. Second branchial cleft cysts: variability of sonographic appearances in adult cases. AJNR 2000;21(2):315-319.
- Ahuja AT, Wong KT, King AD, Yuen EH. Imaging for thyroglossal duct cyst: the bare essentials. Clin Radiol 2005;60(2):141-148.
- Ahuja AT, King AD, Kew J, et al. Head and neck lipomas: sonographic appearance. AJNR 1998;19(3):505-508.
- King AD, Ahuja AT, King W, Metreweli C. Sonography of peripheral nerve tumors of the neck. AJR 1997;169(6):1695-1698.
- Ahuja AT, Richards P, Wong KT, et al. Accuracy of high-resolution sonography compared with magnetic resonance imaging in the diagnosis of head and neck venous vascular malformations. Clin Radiol 2003;58(11):869-875.
Newsletter
Stay at the forefront of radiology with the Diagnostic Imaging newsletter, delivering the latest news, clinical insights, and imaging advancements for today’s radiologists.
Advertisement
Related Content
Advertisement

Latest CME








Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Leading Breast Radiologists Discuss the Recent Lancet Study on AI and Interval Breast Cancer
2
FDA Clears AI-Powered Triage Platform for Digital Breast Tomosynthesis
3
Is AI Better Than Neuroradiologists at Evaluating Aneurysm Growth on CTA and MRA Scans?
4
Radiology Roundup of New FDA Clearances — February 1 — February 7
5