What a New CCTA Study Reveals About the Larger Picture of Assessing Patients with Chronic Coronary Syndrome
Emerging CCTA research affirms the importance of going beyond LDL reduction in the evaluation and treatment of patients with chronic coronary syndrome.
Recently published research on residual coronary atherosclerotic risk and low LDL-cholesterol in patients with chronic coronary syndrome (CCS) is quietly dangerous. It’s not wrong but it can be misunderstood.
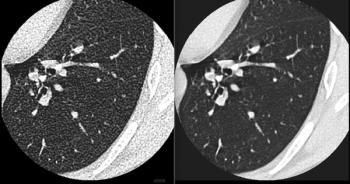
Let’s go straight to the core. What the study actually shows is that in 479 CCS patients undergoing coronary computed tomography angiography (CCTA), lower LDL-C (< 7 0 mg/dL) was associated with more severe coronary artery disease (CAD) and higher plaque burden.1
What was even more interesting is that these patients had more metabolic syndrome, worse glucose metabolism markers and more diabetes/pre-diabetes. Diabetes (OR ~6.1) and pre-diabetes remained strong independent predictors of CAD risk.1
The uncomfortable observation is that the “best treated” patients (low LDL) had the worst arteries.
However, before anyone panics, this is not saying LDL reduction is harmful. This is saying something much more subtle and more important.
What is really happening?
1. Reverse causality (the elephant in the room). Patients with prior events, higher baseline risk and more aggressive treatment end up with lower LDL. Low LDL is a marker of treated high-risk patients, not the cause of disease.
2. Metabolic risk is the real signal. The study shows very clearly that glucose dysregulation dominates residual risk. Diabetes, pre-diabetes, insulin resistance and metabolic syndrome are strongly associated with plaque burden and Leiden score.1
This is the key shift. For years, we simplified CAD risk to: LDL = bad and lower LDL is better. That’s still true but incomplete. What this paper actually teaches is that you can have “perfect LDL” and still have high atherosclerotic risk. Atherosclerosis does not hinge on cholesterol alone. Atherosclerosis involves a combination of metabolic factors, inflammatory factors and vascular disease.
What’s the imaging angle (the real gold here)?
CCTA shows more non-calcified plaques in the low LDL group, higher plaque burden (SIS) and higher Leiden risk scores. This is exactly where imaging becomes decisive: Biology > numbers.1
The clinical implication (the part guidelines are still catching up with) is that treating LDL alone does not eliminate risk because residual risk involves a combination of metabolic, inflammatory and phenotypic factors.
This paper reinforces a concept that is still underused clinically. CAD is an atheroma disease, not a cholesterol disease.
What’s the real mistake to avoid? A superficial reading would lead to an assumption that “Low LDL is associated with more disease, so LDL doesn’t matter.” That would be wrong. The correct interpretation is that LDL reduction works but it does not address the whole disease.
This is exactly where advanced CCTA (plaque quantification, phenotype), photon-counting CT (microstructure, composition) and artificial intelligence (AI)-based quantitative computed tomography (AI-QCT) will redefine risk stratification.
The bottom line is that LDL reduction is necessary but absolutely not sufficient. If you only track LDL, you are managing a number, not the disease.
Reference
- Neglia D, Pane K, Occhipinti M, et al. Residual coronary atherosclerotic risk and low LDL-cholesterol in chronic coronary syndromes. Eur Heart J Imaging Methods Pract. 2026 Feb 4;4(1):qyag021. Doi: 10.1093/ehjimp/qyag021. eCollection 2026 Jan.
Dr. Cademartiri is the director of advanced cardiovascular imaging and photon-counting CT at the Scientific Institute for Research, Hospitalization, and Healthcare Synlab Diagnostic Network in Naples, Italy. He is also a consultant in advanced cardiovascular imaging at CDI/Centro Diagnostico Italiano in Milan, Italy.
(Editor’s note: This blog is adapted with permission from Dr. Cademartiri’s original LinkedIn post at:
Related Content