|Articles|December 14, 2009
Diagnostic Imaging Europe
- Diagnostic Imaging Europe Vol 25 No 8
- Volume 25
- Issue 8
MRS, perfusion MRI separate radiation necrosis from tumor
Radiation plays an important role in the treatmentof primary and secondary centralnervous system neoplasms.
Advertisement
Radiation plays an important role in the treatment of primary and secondary central nervous system neoplasms. External-beam radiotherapy and gamma knife radiosurgery have become essential tools for managing these tumors.
Increasingly aggressive treatment protocols are being used in the hope of improving patient survival rates. These regimens, however, can lead to a wide spectrum of complications owing to the overlap between “effective” and “neurotoxic” doses of radiation. Differentiating tumor recurrence from treatmentinduced change is a clinical and radiological challenge.
Researchers have suggested three mechanisms to explain radiationinduced neurotoxic effects in the brain:
• Direct cellular damage. Radiation generates reactive oxygen species that damage cellular DNA, eventually leading to the induction of cellular apoptosis. Tumor cells with a high mitotic rate are affected the most because they are less able than normal cells to instigate DNA repair.
Healthy cells can undergo radiation-induced apoptosis too, the most sensitive being oligodendrocytes, endothelial cells, and subependymal cells. Neurons are relatively insensitive to radiation-induced damage.1-3
• Vascular damage. Hyalinization, wall thickening, and fibrosis of irradiated vessels result in accelerated atherosclerosis with potential vascular obstruction and thrombosis. The endothelial damage and increased vascular permeability can also disrupt the blood-brain barrier.1,4
• Inflammatory and immunologic phenomena. Cellular death and tissue destruction induces an immunologic response that results in reactive gliosis, endothelial proliferation, and other inflammatory changes. A complex scenario is generated and a vicious destructive cycle is set up.5
DIAGNOSTIC DILEMMA
Normal parenchyma close to target neoplasms can receive highs doses of radiation, resulting in edema, demyelination, and radiation necrosis. Radiation necrosis is the most severe of these radiation-induced injuries. This complication, which is secondary to coagulative necrosis of the brain, generally affects white matter at the site of the primary tumor. It is irreversible, often progressive, and fatal.5-7
Distinguishing between radiation necrosis and tumoral recurrence presents clinicians and radiologists with an important diagnostic challenge. Both conditions occur within two years of radiation therapy, and morphological features are often unspecific. Symptoms associated with radiation necrosis are also unspecific. These include seizures, focal neurologic deficits, personality changes, memory loss, dementia, and/or reemergence of the initial tumor symptoms. Radionecrosis at the resected tumor bed may consequently mimic recurrence, while any radiation-induced lesions detected distant to the primary tumor site may be misinterpreted as multifocal glioma.6
But accurate diagnosis is essential, not least because the prognosis and treatment for radiation necrosis and tumor recurrence vary greatly. The modalities used most commonly to diagnose and follow up patients with brain tumors, CT and conventional MRI, are often insufficient. Advanced MRI techniques, such as perfusion imaging and spectroscopy, are needed instead.
Alternative imaging methods for the differential diagnosis of radiation necrosis and tumoral recurrence include thalium-201 SPECT and FDGPET. These techniques are expensive and not widely available. Carbon-11- methionine (MET) PET offers high specificity for the detection of tumor recurrence, but this technique is available only in academic research centers at present.8
CONVENTIONAL MRI
Morphologic features of radionecrosis seen on conventional MRI include mass effect, vasogenic edema, and contrast enhancement. These features are all similar to those exhibited by a malignant tumor. Radiation necrosis may additionally progress and increase in size, leading to a dangerous mass effect, just like a neoplasm.
Some morphological features help identify radiation necrosis. These include some special enhancement patterns, cystic changes, and periventricular white matter involvement. Peripheral enhancement in necrotic tissue, which can result from bloodbrain barrier disruption, cannot be used to differentiate radiation damage from recurring tumor. Some authors have, however, described specific enhancement patterns, “Swiss cheese” or “soap bubbles,” for example, that reflect the central necrotic area in radiation- induced lesions (Figure 1).6 The appearance of newly enhanced foci, either in or adjacent to irradiated and previously unenhanced tumor, often constitutes radiation necrosis; less frequently it indicates progression to a high-grade tumor.6
Lesions due to radiation necrosis have a predilection for periventricular white matter involvement, particularly next to the ventricle horns. This is because oligodendrocytes and the areas that are less vascularized are more susceptible to irradiation. Radiologists should remember that radiation necrosis may appear anywhere, so long as it is within the field of irradiation.5,6
The development of cystic changes and a reduction in lesion volume may be identified on serial images as radionecrosis evolves, particularly after treatment with corticosteroids. In the vast majority of cases, however, morphological features are not sufficient to rule out residual tumor. Definitive diagnosis requires biopsy and/or complementary imaging studies.
ADVANCED IMAGING
Advanced imaging techniques, such as spectroscopy and perfusion, have improved the evaluation of brain tumors on MRI. These techniques make it possible to study vascularization (through tissue perfusion) and build a metabolic profile of brain lesions. Conventional MRI studies can provide only anatomic or structural information. These additional physiological parameters may help radiologists differentiate radiation necrosis from recurrent tumor.
Perfusion MRI allows the study of cerebral blood volume (CBV), that is, the volume of blood passing through the brain. Tumoral cells stimulate the formation of new vessels, which are histologically abnormal and more permeable than normal brain vessels. These histologic and angiographic abnormalities result in increased blood volume and vascular flow.
CBV is usually measured in mL/ 100 g tissue. Images obtained with a gradient echo echoplanar technique before, during, and after gadolinium injection can be used to create a CBV map of the brain.9 Radiologists can then use these maps to distinguish between hypervascularized tumoral lesions and tissue that has become hypovascularized following radionecrosis.9-11
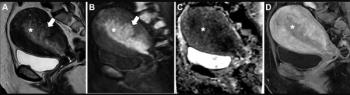
Intermediate perfusion values, similar to those of white matter, are observed more often in cases of radiation necrosis (Figure 2). Tumor recurrence, on the other hand, is generally associated with high perfusion values that are similar to those of gray matter (Figure 3).
Perfusion MRI has demonstrated high utility in the diagnosis of highgrade malignant neoplasms. Studies have shown a good correlation between CBV maps and histologic and angiographic vascularities in gliomas.10,11 CBV maps generated from perfusion MRI studies can also offer an indication of outcome in patients with cerebral metastases prior to treatment with linear accelerator radiosurgery. Perfusion MRI may consequently be a valuable adjunct to conventional MRI.12
Proton MR spectroscopy provides metabolic and chemical information about brain lesions.13-15 It essentially offers in vivo chemical spectra of tissue that reflect ongoing metabolic activity in target lesions; e.g., cellular necrosis, gliotic changes, or proliferation of neoplastic processes.13,14 Results from MRS may be comparable to those from FDG-PET.14
Single- and multivoxel techniques may be used when performing MRS. The point-resolved spectroscopy sequence (PRESS) is used most often in daily practice for volume selection. Various metabolic markers may be measured. Choline (Cho) levels reflect the membrane metabolism that is associated with cellular turnover. Nacetyl- aspartate (NAA) functions as a neuronal cell marker, while creatine (Cr) indicates cellular bioenergetics. Lipid-lactate (lip-lact) peaks are present in necrotic tissue and reflect anaerobic metabolism.
Chemical patterns can then be observed that correlate with different types of lesions. Spectra with elevated Cho and diminished NAA levels tend to be associated with aggressive neoplasms. Radiation necrosis, on the other hand, typically presents on MRS with decreased levels of Cho, NAA, and Cr, and observed liplact peaks (Figure 4).
Cho and Cho/Cr are considered to be the most useful markers for the differentiation of neoplasms from radiation necrosis on MRS. Moderate levels of Cho and/or a Cho/ Cr index of less than 1.3 are observed more frequently in radiation necrosis (Figure 5). Elevated Cho levels and/or a Cho/Cr index greater than 1.3 is more suggestive of a malignant tumor.13
The postradiotherapy landscape is, however, extremely complex. Irradiated tissues may undergo several coexisting processes, including progressive cellular necrosis and gliosis, inflammatory changes, and reactive glial cell proliferation. A mixture of radiation-induced changes and residual tumor will also be observed in around one-third of cases.9,15 MRS and perfusion MRI findings will consequently be complex too. For example, cellular necrosis and reactive glial cell proliferation may translate into increased Cho levels on MRS,13 while endothelial proliferation may appear as highly vascularized areas on perfusion imaging.9
A combination of MRS and perfusion MRI may help distinguish between radionecrosis and recurrent tumor. We have identified two patterns associated with radiation necrosis as follows:
• Initial phases (cellular necrosis and reactive mechanisms coexist). moderate increase in Cho and Cho/Cr index < 1.3; moderate to low perfusion.
• Later phases (cellular necrosis predominates). increased lip-lact levels; decreased levels of all other metabolites; low perfusion.
ADDITIONAL FACTORS
A number of factors are involved in the development of radiation necrosis. For example, the patient's age is important. Children's brains are more vulnerable to radiation than adult brains.16 Tissue and cellular susceptibility also plays a part. Cells with a high mitotic rate and tissues with a relatively poor blood supply are more sensitive to radiation damage.
Radiologists must remember that radiation necrosis may appear anywhere, but that the site will always fall within the irradiated volume. The total radiation dose that can be tolerated by the brain is 60 to 70 Gy. Cerebral necrosis is unlikely at doses below 50 to 54 Gy delivered over 25 fractions, or when the fractional dose is < 2 Gy.16-19
Patients who have received a total dose of 45 to 50 Gy have a 5% chance of radiation necrosis.16 The higher the dose, the shorter the delay in radiation necrosis developing. The risk of radiation necrosis rises if the fractionation daily dose is greater than 2 Gy.18-20
Vasculopathic risk factors, diabetes mellitus or hypercholesterolemia, for instance, increase the risk of radiation necrosis. Adjuvant chemotherapy shortens the latency period and increases the risk of radionecrosis developing.19
In conclusion, radiation-induced changes in the brain occur more frequently than they used to and tend to be more severe owing to the increased use of radiation therapy and more aggressive treatment protocols. Morphologic features seen on conventional followup imaging studies are nonspecific and are not sufficient to rule out residual or recurrent tumor.
Advanced MRI techniques can help radiologists distinguish between radiation necrosis and tumoral recurrence. A complete assessment should also take account of variables related to the therapy, the patient's age and health, and morphological findings.
Articles in this issue
over 16 years ago
Teleradiology promises real benefits for radiologistsover 16 years ago
Better clinical coding saves valuable time and moneyover 16 years ago
C-11 Cho PET/CT helps localize prostate cancer recurrenceover 16 years ago
Case of the Issueover 16 years ago
Dual-source technology extends CT applicationsover 16 years ago
Spain emerges out of wildernessto match elite in Europeover 16 years ago
Research study validates use of BI-RADS in breast MRIAdvertisement
Related Content
Advertisement












Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Can Contrast-Enhanced Mammography Improve Breast Cancer Staging?: Nine Takeaways from a New Literature Review
2
What Does the Future Hold for Nuclear Medicine?
3
New CCTA Study Suggests that Current Plaque is the Key Biomarker for Assessing MACE Risk
4
Breast Cancer Screening: Where Things Stand
5