
|Articles|November 9, 2009
Diagnostic Imaging Europe
- Diagnostic Imaging Europe Vol 25 No 7
- Volume 25
- Issue 7
Microbubble agents helppinpoint renal lesions
Author(s)Maria E. Sellars, MBBS, Paul S. Sidhu, MRCP
Ultrasound is often the preliminary investigation for many diseases affecting the kidney.
Advertisement
Ultrasound is often the preliminary investigation for many diseases affecting the kidney. The examination is safe, inexpensive, and widely available. Most investigators will refer the patient for CT or MRI if a focal abnormality is found. Contrast-enhanced ultrasound, however, may be a feasible alternative as a problem-solving tool when suspected renal pathology is found.
Contrast-enhanced ultrasound has become established in routine clinical practice for liver disease and its use is expanding into other areas. Published guidelines are available on the modality’s use for the characterization of focal liver lesions as well as its role in other intra-abdominal organs, including the kidney.1
This imaging method offers several practical advantages. Ultrasound contrast agents are simple to use and are well tolerated by patients.2 Real-time imaging often allows a diagnosis to be made promptly. No ionizing radiation is involved, there is no risk of patients suffering claustrophobia, and the cost of the examination is lower than that for CT or MRI. Contrast-enhanced ultrasound may also provide supplementary information not evident on other modalities.
Ultrasound contrast agents consist of air or perfluorocarbon gas microbubbles that are stabilized by a protein, lipid, or polymer shell. The microbubbles typically measure less than 7 ìm in diameter, making them small enough to cross capillary beds but too large to enter interstitial fluid. These properties enable the microbubbles to serve as blood pool agents.
Microbubble contrast agents survive passage through the cardiopulmonary circulation and typically remain in the vascular compartment for six to eight minutes after intravenous injection. This stability allows sufficient time for imaging. The principal agent used in Europe is SonoVue (Bracco), which is composed of a sulfur hexafluoride gas with a phospholipid shell. The microbubbles are metabolized by the liver and the gas is exhaled via the lungs. Other available agents include Definity (Bristol-Myers Squibb), composed of octafluoropropane gas encapsulated in an outer lipid shell, and Optison (GE Healthcare), which has an albumin shell and an octafluoropropane gas core.
We use SonoVue for our contrast-enhanced renal ultrasound work. The microbubbles are administered in a suspension of saline which, once prepared, remains stable for several hours. An adult patient will typically receive 2.4 mL of the microbubble/saline solution, injected manually through an arm vein. This is followed by a 5 to 10 mL saline flush. Further doses of 2.4 mL may be administered as required, and there is no recommended maximum dose. In a phase I study, doses of up to 56 mL of SonoVue were administered to normal volunteers without adverse events, and no signs or symptoms of overdose have been identified to date. Although we have experience using contrastenhanced ultrasound in pediatric liver lesions, currently we do not use the technique for assessment of pediatric renal lesions.
Examinations are performed on an Acuson Sequoia (Siemens Medical Solutions) machine, using the cadence contrast pulse sequence (CPS), low mechanical index (MI) technique. Examinations of the kidney are quick, continuous, and can be repeated for several minutes. The examination is not associated with nephrotoxicity and can be used safely in cases of renal failure and obstruction.
CONTRAST DYNAMICS
Some understanding of the dynamics of ultrasound contrast within the kidney is essential when using this modality. Microbubble agents remain entirely intravascular, unlike iodinated and paramagnetic contrast agents. Because they are not excreted by the kidneys, there is no nephrographic or excretory phase.
The enhancement pattern of the kidney, which has a single afferent blood supply, is different from that seen in the liver, which has a dual blood supply. Distinct enhancement phases may be identified in the renal parenchyma. The early arterial corticomedullary phase with corticomedullary differentiation lasts 20 to 40 seconds. A late corticomedullary phase, in which homogenous enhancement is seen in both the renal cortex and medulla, lasts 45 to 120 seconds.
The low MI technique is used almost exclusively when generating renal images. This technique minimizes microbubble destruction, allowing real-time observation throughout the period that microbubbles are present in the blood pool. Low MI pulse inversion imaging causes normal tissue echoes to be suppressed. The baseline precontrast image appears dark and echoes from the microbubble contrast are enhanced. All postcontrast echogenicity is consequently attributed to the presence of microbubbles.
Highly vascular lesions appear echogenic with respect to the adjacent renal parenchyma, reflecting the increased number of microbubbles in their vascular pool. Nonvascular lesions appear black.
TUMORS, PSEUDOTUMORS, CYSTS
Contrast-enhanced ultrasound may be of value when evaluating anomalies in lobar anatomy that simulate tumors on baseline ultrasound. The column of Bertin is a good example. This normal renal structure comprises nonreabsorbed polar parenchyma of one or both subkidneys that fuse to form a normal kidney. Its location between overlapping regions of two renal sinus systems, the presence of normal renal tissue, and the observation of a smooth surface contiguous with adjacent parenchyma should enable differentiation from tumor.
Fetal lobulation and lobar dysmorphism may also be misinterpreted as focal lesions.3 The suspicious area should remain isoreflective to normal renal parenchyma in all phases of enhancement following administration of microbubble contrast (Figure 1), reassuring physicians and patients alike.4
Renal cysts are generally assessed by radiologists and urologists according to the Bosniak classification, which is based on the analysis of specific CT features.5 Simple (type I) or minimally complicated (type II) cysts appear on B-mode ultrasound as unilocular, echofree structures of varying size, either within the substance or at the margin of the kidney. Simple cysts remain dark after microbubble contrast enhancement, even if they contain echoes on baseline ultrasound. The result is that simple cysts, and particularly small ones, are more conspicuous on contrastenhanced ultrasound. This suggests that microbubble contrast could be useful in the early detection of conditions such as polycystic kidney disease.
Another practical role for renal contrast- enhanced ultrasound is to evaluate lesions that are equivocal on CT and cannot be distinguished from malignant tumors (Bosniak type III cysts), namely by aiding the delineation of internal architecture. Microbubbles can be visualized in real-time within the fine capillaries that supply the cyst walls and internal septa. This allows suspicious features that may not be evident on CT, such as septations or mural nodule enhancement, to become more apparent. 6,7 Contrast-enhanced ultrasound is also superior to unenhanced ultrasound and contrast-enhanced CT in the diagnosis of malignancy in complex cystic renal masses.8
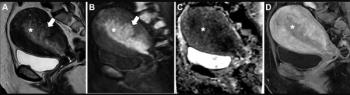
The main advantage of contrastenhanced ultrasound in overtly malignant cysts (Bosniak type IV) is to add to CT or MRI findings. Microbubbles can be employed to further characterize the tumor, and to distinguish solid components from cystic and necrotic parts that do not enhance (Figure 2).
The value of contrast-enhanced ultrasound in renal tumor characterization is currently limited. Benign and malignant tumors can exhibit varying enhancement patterns, and there are no exact criteria to distinguish between the two groups. This task continues to be performed predominately on CT and/or MRI.
True tumors usually show a disparity in enhancement after administration of microbubble contrast, unlike pseudotumors that have homogenous enhancement patterns identical to the adjacent renal parenchyma.
Solid renal cell carcinomas less than 3 cm in diameter often show diffuse, heterogeneous enhancement during the early corticomedullary phase, frequently with a hypervascular appearance. Enhancement may, alternatively, be homogenous, though this is less common.9 Cystic or avascular necrotic components appear black, making them more noticeable (Figure 3).
Microbubble agents are limited in the assessment of renal cell carcinoma. RCC can have arterial-phase contrast enhancement similar to adjacent renal parenchyma, making the tumors less evident after microbubble injection. Renal hypovascular metastases, on the other hand, have a persistent hypoech-oic appearance after microbubble injection that might aid diagnosis.9
Contrast-enhanced ultrasound may be used to distinguish between lesions that may be characterized on ultrasound alone, such as minimally complicated cysts, hyperechoic or hemorrhagic cysts simulating a renal tumor, pseudotumors, and those lesions that will need additional investigation on cross-sectional imaging.
INFARCTION, INFECTION, TRAUMA
Contrast-enhanced ultrasound allows renal perfusion defects to be interpreted with confidence. Perfusion defects appear as single- or multifocal, wedgeshaped areas of absent, diminished, or delayed enhancement when compared with adjacent renal parenchyma (Figure 4).
This technique may be of particular use after renal transplantation. Microbubble imaging can also facilitate the diagnosis of arterial and venous thrombosis as well as postinterventional complications such as hematomas, arteriovenous shunts, and false aneurysms.
Abscesses formed by renal infection can be identified by the central liquid portion of the abscess and will show a lack of enhancement as intralesional vessels are destroyed or displaced by the colliquative process. Fine internal septa may develop as the abscess evolves, and they become more obvious on ultrasound following contrast administration (Figure 5).
CT is undoubtedly the modality of choice for assessment of visceral and skeletal injuries in high-velocity trauma. Contrast-enhanced ultrasound may have a role, however, in stable patients with low-energy blunt trauma as an aid to FAST scanning and for followup. The absence of ionizing radiation means that this strategy may be especially useful in pediatric patients.
Microbubble imaging has been shown to be more sensitive than Bmode ultrasound and almost as sensitive as CT in the detection of solid organ injury in blunt abdominal trauma. 10 The renal parenchyma normally enhances intensely following contrast administration. Hematomas or lacerations are avascular and appear as hypoechoic lesions (Figure 6).
In conclusion, contrast-enhanced ultrasound is a valuable addition to radiologists’ armory, enabling increased confidence in the diagnosis of renal pathology. It is a repeatable, real-time, multiplanar imaging modality that uses a completely intravascular contrast agent. The method is noninvasive, involves no exposure to ionizing radiation, and may be used in patients with renal impairment and those who cannot be examined with contrast-enhanced CT and/or MRI. Recognition of specific enhancement features is, however, essential.
Articles in this issue
over 16 years ago
MR guidance prepares to enter endovascular realmover 16 years ago
Intrapancreatic accessory spleenover 16 years ago
MRI cracks down on 'age doping' in international youth sportsover 16 years ago
Nuclear medicine society includes Europe in clinical trials networkover 16 years ago
Mammography shifts toward spectral imagingover 16 years ago
Recent events at WHO prove bigger is not always betterover 16 years ago
Researchers grapple with dose reduction methods in cardiac CTover 16 years ago
Global flu epidemic poses possible threat to RSNAover 16 years ago
Spider fossils! See them in 3D CT!over 16 years ago
Ultrasound predicts metastases, survival of patients with melanomaAdvertisement
Related Content
Advertisement












Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Can Contrast-Enhanced Mammography Improve Breast Cancer Staging?: Nine Takeaways from a New Literature Review
2
What Does the Future Hold for Nuclear Medicine?
3
Breast Cancer Screening: Where Things Stand
4
New CCTA Study Suggests that Current Plaque is the Key Biomarker for Assessing MACE Risk
5