
|Articles|July 18, 2013
Low-Dose CT Lung Cancer Screening Best for Highest Risk Patients
Author(s)Leah Lawrence
Low-dose CT lung cancer screening was most beneficial in the 60 percent of people who had the highest likelihood of dying from the disease.
Advertisement
Screening for lung cancer with low-dose computed tomography (CT) was the most beneficial in people who had the highest likelihood of dying from the disease, according to data taken from participants in the National Lung Screening Trial (NLST).
In fact, 88 percent of the deaths prevented by screening were among the 60 percent of participants classified as being at the highest risk for lung-cancer death using predictors including demographic and clinical risk factors for the disease.
“The findings provide evidence for outside organizations who are interested in developing risk-based lung screening recommendations,” Hormud A. Katki, PhD, from the division of cancer epidemiology and genetics at the National Cancer Institute, told Diagnostic Imaging. Katki and colleagues published the findings in
Current data show that lung cancer is the most common cause of cancer-related death in the United States, accounting for more than 25 percent of all cancer deaths. Previously published data from the NLST indicated that low-dose CT screening reduced lung cancer death among a population of heavy smokers.
“We wanted to determine which participants in the NLST might receive the greatest benefit from screening,” Katki said. “To do this, we calculated each NLST participant’s risk of lung cancer death in the NLST. We then calculated the number of prevented lung cancer deaths from LDCT lung screening.”
Katki and colleagues calculated the number of false positive results and lung-cancer deaths prevented among the 26,604 participants in the trial who underwent screening with CT. The participants were then placed into quintiles of five-year lung cancer death risk.
“Not surprisingly, we found that smokers with the highest risk of lung cancer had the most benefit from low-dose CT,” Katki said.
With each increasing risk quintile, the number of prevented lung cancer deaths per 10,000 person-years increased, from 0.2 in the lowest risk quintile to 12 in the highest quintile. When the researchers calculated a ratio of the number of participants with false positive results to the number of screening-prevented deaths, they found that the number decreased across risk quintiles with 1,648 for the lowest risk quintile and 65 for the highest risk quintile.
Only 1 percent of low-dose CT prevented lung-cancer deaths occurred among the 20 percent of participants who were at lowest risk.
“Although there is currently a consensus among published screening guidelines on recommending low-dose CT screening for patients who meet the NLST entry criteria, some experts have speculated that further refinement of selection criteria may be appropriate,” Katki and colleagues wrote. “Our results confirm that tailoring of low-dose CT screening to a patient’s predicted risk of lung-cancer death could narrow the NLST-eligible population without a loss in the potential public health benefits of screening or a disproportionate increase in the potential harms.”
The researchers specified that the results of this study must be interpreted within the context of using low-dose CT in the NLST. In addition, they acknowledge that this study did not take into account other potential harms of CT screening including “psychological burden of false positive results, complications with invasive follow-up procedures, and radiation-induced cancers.”
Newsletter
Stay at the forefront of radiology with the Diagnostic Imaging newsletter, delivering the latest news, clinical insights, and imaging advancements for today’s radiologists.
Advertisement
Related Content
Advertisement

Latest CME










Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Molecular Imaging in Focus: Emerging Insights on the PET and SPECT Imaging Agent 61Cu-NU101 for PCa
2
The Inflection Point for AI in Radiology: Emerging Insights for 2026
3
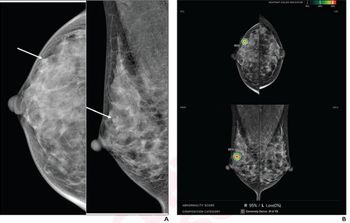
Mammography Study Assesses Ability of AI to Predict DCIS Recurrence After Breast Surgery
4
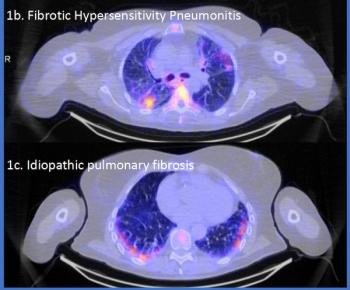
SPECT/CT Agent Garners FDA Fast Track Designation for Inflammation Assessment in Interstitial Lung Disease
5