|Articles|December 26, 2014
Mixed Messages About Breast Density As Risk Factor
Author(s)Whitney L. Jackson
Breast density notification legislation has amped up the discussion about breast cancer screening but may be delivering mixed messages.
Advertisement
CHICAGO - As of July 2014, 32 states either had a breast density notification law or were working on
According to industry experts at this year’s Radiological Society of North America meeting, new cancers are being found, but radiologists have learned something else in the process. Dense breast tissue doesn’t necessarily raise a woman’s risk of breast cancer – instead, it more directly affects the sensitivity of the test she receives.
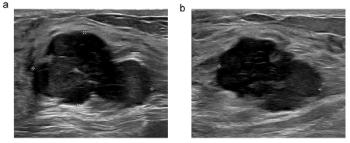
“The increased rate of breast cancers in dense tissue is largely due to masking – the obstruction of the cancer by the dense tissue,” said Stephen Feig, MD, a radiologist at the University of California-Irvine with an interest in breast screening guidelines and controversies. “Dense breast tissue is much less associated with an actual higher risk of developing the disease than was originally anticipated.”
The common belief is that women with dense breasts are four times as likely as other women to develop breast cancer, said Barbara Monsees, MD, women’s health professor in the diagnostic radiology divisions at Washington University School of Medicine in St. Louis. But, she added, it’s a misleading assertion.
Women with scattered or heterogeneous breasts have a breast cancer relative risk of one. For women with fatty tissue and dense tissue, the relative risk is one-half and two times, respectively. So, while a woman with dense breasts is four times as likely as a woman with fatty breasts to have a breast cancer identified, that relative risk can’t be assigned to all women.
Mammography remains the gold standard for detecting breast cancer, and results of the breast density notification legislation have shown supplemental ultrasound screening does detect
Consequently, a growing number of institutions are looking into the feasibility of a fast three-minute MRI. Facilities are also increasing their use of digital mammography and tomosynthesis to identify more breast cancers.
It’s still imperative, though, that women be informed of their breast density, she said.
“Women should know their breast density so that, most important of all, they can begin the discussion with their physician about all their other risk factors,” Monsees said. “If there are other risk factors, such as a personal or family history of breast cancer, then density might elevate the risk. It’s an important discussion to have, and if knowing their breast density launches that conversation, then this is a big benefit.”
And, there are far greater risk factors that women face, Feig said. A personal and family history increases risk two-to-four times, and having a mother and sister who both had breast cancer presents a four-times risk.
Unfortunately, he said, the emphasis on breast density is being used to promote a form of personalized screening that could put some women at risk. One suggestion points to screening women age 40 and older who have dense tissue every year with MRI and, potentially, ultrasound. However, the same recommendation promotes screening all other women every two-to-four years because of their presumed lower risk due to lower density and no family history.
“This was written about in the
Delivering mammography services in this type of personalized or risk-based way could be dangerous, he said, because 80% of women diagnosed with breast cancer have no known risk factors.
Overall, Monsees said, the breast density notification law has proven to simply be a good starting point for the radiology community.
“Density alone isn’t enough information to allow a woman to make a decision about what to do and how to go forward. If we do have a federal law dealing with this, we want one that looks at the entire package,” she said. “The biggest risk factor is family history, and I can’t tell you how many women don’t know that. It’s a sad commentary about the kind of communication that exists. We need to elevate the level of discussion.”
Advertisement
Related Content
Advertisement














Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Emerging PET Radiotracer May Enhance Detection of Small Metastases in Patients with Advanced Melanoma
2
Can Biomechanical CT Have an Impact in Opportunistic Screening for Osteoporosis?
3
Can Photon-Counting CT Provide Timely Clarity After Mechanical Thrombectomy?
4
What a Meta-Analysis Reveals About FAPI PET/CT for Detection of Peritoneal Metastases
5