|Articles|January 3, 2012
Interventional Radiology Costs Less, Safer than Surgery for PAD
Author(s)Diagnostic Imaging Staff
Endovascular lower-extremity revascularization procedures performed by interventional radiologists bring about less transfusion and intensive-care unit use, shorter hospital stays, fewer repeat revascularization procedures, fewer amputations, and lower costs compared to those done by vascular surgeons.
Advertisement
Endovascular lower-extremity revascularization procedures performed by
So concludes a
Authors said this study is the first and largest of its kind on peripheral arterial disease (PAD) treatments for Medicare patients age 65 and older. PAD is a narrowing of the blood vessels in the leg, which limits the supply of oxygen and nutrients to the leg, causing pain and discomfort. It affects an estimated 10 million people in the United States (12 percent to 20 percent of Americans over age 65) and can lead to heart attack or stroke.
The team found the potential cost savings to be substantial.
"We noted that the adjusted average one-year procedure cost when performed by interventional radiologists was about $17,640. That's a cost savings to Medicare of approximately $1,000 per procedure – which means that in such a large population, treatments for PAD by interventional radiologists could potentially save taxpayers $230 million each year. And the patient outcomes are better," said Timothy Murphy, MD, an interventional radiologist and director of the Vascular Disease Research Center at Rhode Island Hospital in Providence.
Murphy and colleagues reviewed Medicare claims data from more than 14,000 patients with PAD from 2005 to 2007 from Medicare's Standard Analytical Files, a large dataset that contains all services (physician, inpatient, and outpatient). The authors compared outcomes of percutaneous PAD treatments in Medicare patients according to the physician specialty type (interventional radiologist, interventional cardiologist, vascular surgeon) and assessed mortality, transfusion, intensive care use, length of stay, and subsequent restoration of blood supply or amputation.
Murphy said the study provided strong evidence that treatment by interventional radiologists provides numerous benefits to the PAD patient, such as less risk of infection, less anesthesia, less pain and scarring, faster recovery and a quicker return to normal activities.
“The Medicare data clearly show more transfusion and intensive care utilization, longer length of stay, more repeat procedures or amputations and higher costs when treatment is not performed by interventional radiologists," Murphy said.
Advertisement
Related Content
Advertisement













Advertisement
Advertisement
Trending on Diagnostic Imaging
1
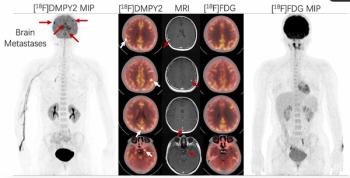
Emerging PET Radiotracer May Enhance Detection of Small Metastases in Patients with Advanced Melanoma
2
Can Biomechanical CT Have an Impact in Opportunistic Screening for Osteoporosis?
3
Can Photon-Counting CT Provide Timely Clarity After Mechanical Thrombectomy?
4
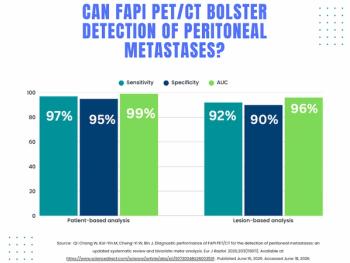
What a Meta-Analysis Reveals About FAPI PET/CT for Detection of Peritoneal Metastases
5