
|Articles|April 1, 2020
COVID-19 and Lung Ultrasound: Experts Suggest New International Standards
Author(s)Whitney J. Palmer
Recommendations based on the experiences of Italian providers.
Advertisement
As more cases of COVID-19 are being diagnosed, the body of radiological data to support the use of lung ultrasound in managing patients with the infection also continues to grow.
Medical experts from Italy – the country hardest hit by COVID-19 second only to the United States – compiled their experiences and advice for using lung ultrasound, creating a standardized approach that could be implemented in hospitals and clinical worldwide.
Their expertise and guidance on equipment use, disease classification, procedures, and data sharing were published on March 30 in the
“COVID-19 is a worldwide health challenge, involving not only health, but also economics and social behaviors,” wrote the authors, led by Gino Soldati, M.D., from Valle del Serchio General Hospital’s Diagnostic and Interventional Ultrasound Unit. “For the first time in the era of modern medicine, the whole world is facing the same threat. This can give us the opportunity to change our research approach. Time has probably come to share our knowledge and planning the best care all together.”
Equipment
To reduce contamination and promote sterilization, a wireless probe and tablets are the most appropriate ultrasound equipment because they can be easily wrapped in single-use plastic covers, they recommended. These devices are also less expensive than more traditional machines. Portable machines can be used if wireless equipment is unavailable, but they must be strictly dedicated to COVID-19 patients. Maximum sterilization procedures must be followed for cases, probe, and keyboard covers.
Protocol
When scanning patients, they advised, 14 areas – three posterior, two lateral, and two anterior – should be scanned for 10 seconds each. Scans should be intercostal and cover the widest surface area possible in one scan.
If patients aren’t able to sit upright, particularly those in critical care, sonographers should concentrate on having a partial view of the posterior basal areas. These, they advised, are considered “hot areas” for COVID-19.
In addition:
- Use Convex or Linear probes, according to the patient’s size
- Use single focal point modality (no multi-focusing), setting the focal point to the pleura line
- Keep the mechanical index (MI) low, starting from 0.7 and reducing further, if possible
- Avoid saturation phenomenon as much as possible, control gain, and diminish MI, if needed
- Avoid using cosmetic filters and specific imaging modalities, including harmonic imaging, contrast, doppler, and compounding
- Achieve the highest frame rate possible
- Save data in DICOM format
Disease Scoring
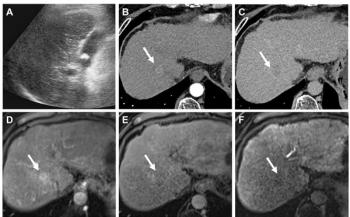
To help classify COVID-19 cases, the researchers suggested scoring the disease burden on a 0-to-3 scale. At the end of each procedure, the sonographer should note the quadrant with the highest score.
Score 3 indicates the most severe findings, such as dense and extended white lung with or without larger consolidations.
Score 2 would include a broken pleura line with small-to-large consolidated areas before the breaking line. Some appearances of white lung could also be visualized.
Score 1 presents an indented pleura line with vertical areas of white below the indention.
For a Score 0, the pleura line is continuous and regular with horizontal artifacts (A-line).
International Database
The global nature of this pandemic has revealed the need for more collaborative sharing of data, images, and artificial intelligence studies, Soldati wrote. In that vein, they encouraged the scientific and medical community to pool resources and create an international database that will hold X-Rays, ultrasound, and CT images from COVID-19 patients.
Related Content:
Such a repository, much like the one recently proposed by the Radiological Society of North America, could facilitate the development of dedicated pattern recognition algorithms that could make identifying COVID-19 easier, as well as allow for comparisons between institutions and the launch of telemedicine programs.
More details about the guidelines are available
Newsletter
Stay at the forefront of radiology with the Diagnostic Imaging newsletter, delivering the latest news, clinical insights, and imaging advancements for today’s radiologists.
Advertisement
Related Content
Advertisement

Latest CME








Advertisement
Advertisement
Trending on Diagnostic Imaging
1
Leading Breast Radiologists Discuss the Recent Lancet Study on AI and Interval Breast Cancer
2
FDA Clears AI-Powered Triage Platform for Digital Breast Tomosynthesis
3
Is AI Better Than Neuroradiologists at Evaluating Aneurysm Growth on CTA and MRA Scans?
4
Radiology Roundup of New FDA Clearances — February 1 — February 7
5